

Personalizing Treatment for Sleep-Related Breathing Disorders
Using the Lamberg Protocol for diagnosis of specific cause(s) and selection of the most appropriate treatment(s) by Steve Lamberg DDS, DABDSM

Dentistry plays a vital role in modern healthcare today, focusing on both oral health and its connection to overall well-being of the individual. Furthermore, dental professionals are increasingly recognized for their ability to identify and address systemic health issues.
Personalized oral and dental care interventions emphasize disease prevention through individualized rather than population-based surveillance, improve diagnosis through more accurate data collection and evaluation, promote earlier detection of abnormalities which helps to avoid further more invasive and expensive treatment, and reduce side effects of mistreatments and delayed treatment.
In most contemporary cultures, diet, exercise, sleep, and breathing are recognized as the essential pillars of overall health and well-being. They are interconnected and influence each other, impacting physical and mental health. As the craniofacial respiratory complex encompasses the structures of the head, face, and oral cavity, and alterations in these structures can directly impact breathing, dentistry finds itself in a unique position to work with the medical community, in a transdisciplinary fashion, to prevent and treat sleep related breathing disorders which affect the overall health of so many people worldwide today.
Sleep related breathing disorders comprise a continuum of conditions from snoring and upper airway resistance syndrome to severe obstructive sleep apnea. Additionally they include central sleep apnea and sleep-related hypoventilation disorders.1
Obstructive sleep apnea (OSA) is a sleep disorder characterized by repetitive episodes of partial or complete obstruction of the upper airway during sleep despite ongoing respiratory efforts. This results in fragmented sleep and intermittent hypoxia.2
Although this disorder is estimated to affect 17% of middle-aged women and 34% of middle-aged men3, a more recent assessment in PubMed and Embase search was used to identify published studies reporting the prevalence of obstructive sleep apnea. This is the first study to report global prevalence of obstructive sleep apnea; with 1 billion people affected, and with prevalence exceeding 50% in some countries. More effective diagnostic and treatment strategies are needed to minimize the negative health impacts.4
For the individual patient, the primary goals for treating sleep related breathing disorders, including OSA, include the following: reduction of health risks associated with breathing disorders, improvement of sleep quality, a decrease in daytime sleepiness and the reduction or elimination of snoring.
As OSA is a sleep related breathing disorder with a high prevalence of comorbidities as well as diverse clinical manifestations and phenotypes, conventional approaches to diagnosis and treatment of OSA are no longer the most effective approach. The debate about what is the best primary treatment between CPAP or OAT was argued at the 2025 AADSM annual meeting and the FLOSAT results were shared prior to publication.5 Novel approaches to measuring the hypoxic burden were also presented including Sleep Apnea Specific Hypoxic Burden “SASHB.” The problem with all of this is that the cause(s) of the disease is not being diagnosed. The only path to optimize treatment of this disease begins with diagnosing the cause for the individual, which is a philosophical shift towards a more personalized approach. The Lamberg Protocol is a treatment algorithm based on addressing the compensations and cause(s) of the disease as a prerequisite to treatment.
This article outlines a workflow from a more proactive screening protocol, because approximately 80–90% of OSAS cases remain undiagnosed6, to a novel “Nextgen” data collection protocol7 which leads to a diagnosis of the cause(s) and recommendations for treatment. It is only when the cause(s) of the SRBD problem is revealed that individualized treatment can be selected for the patient.
This approach is consistent with what Peter Attia refers to as the transition from Medicine 2.0, treating the acute conditions, to Medicine 3.0. Medicine 3.0 reflects a move towards evidence informed vs. evidence based guidelines, adoption of early preventative measures for potentially chronic conditions, and a highly personalized approach to the overall health of an individual patient.8
Dentistry 2.0 is transitioning to Dentistry 3.0 as well. The concept of Orthodontics 3.0 was recently presented by Mike DeLuke DDS, MDS in New York.9 The concept includes examining each patient as an individual rather than an average. Orthodontics 3.0 goes beyond looking at the teeth and includes examination of the face, tongue, airway, behavior and sleep quality. Finally this perspective acknowledges the risk of doing nothing (i.e. “watchful waiting”).
The targeted treatment algorithms in airway compromised dental patients is The Lamberg Protocol. (See figure 1) It is based on addressing specific structural, functional and behavioral compensations and cause(s) of the airway problem rather than the severity index based on frequency of respiratory events, or hypoxic burden during sleep.
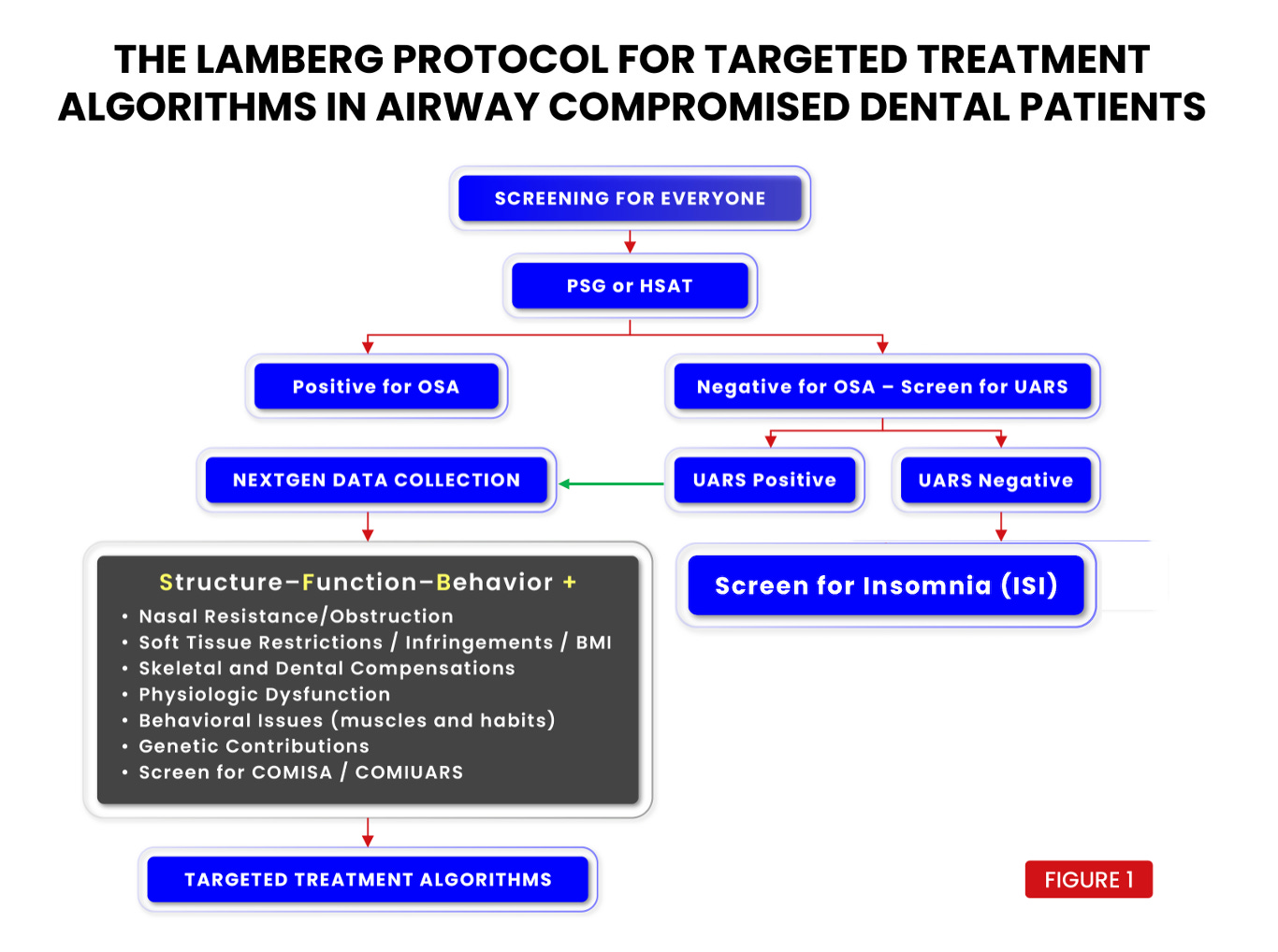
The workflow begins with the Lamberg Questionnaire or “LQ” (See figure 2) for all adults, which is explained in the book, “Treat the Cause…Treat the Airway” (See figure 2a). Children are given the Lamberg Questionnaire of Pediatric Airway and Sleep “LQ-PAS” (see figure 3) When sufficient risk is revealed on the LQ score, the patient is referred for a PSG or HSAT. If the PSG or HSAT is negative for OSA, the patient is evaluated for UARS which is frequently overlooked as RERAs are underestimated in PSG studies and esophageal pressure sensors are infrequently used in clinical laboratory settings.10




Upper Airway Resistance Syndrome “UARS” cannot be overlooked as it may be responsible for health consequences equivalent to or worse than OSA. Untreated UARS can lead to several negative health outcomes including reduced quality of life, increased risk of cardiovascular diseases, hypertension, T2DM and various mental health issues. It can also cause persistent insomnia, daytime fatigue, cognitive impairment and chronic somatic disorders like chronic fatigue syndrome, fibromyalgia and IBS. UARS is defined in general as airflow limitation due to increased respiratory effort leading to arousals from sleep without significant desaturation (i.e., RERAs) associated with daytime symptoms.11 UARS has also been more specifically defined as apnea-hypopnea index < 5 events/h, oxygen saturation ≥ 92%, and respiratory effort–related arousal index ≥5/hour.12 Finally, another study used a slightly different definition when AHI <5/hour, minimum SpO ≥ 92%, the presence of airflow limitation during sleep for ≥5% of total sleep time, and daytime sleepiness and/or fatigue.13 The fact that multiple definitions are used for UARS should not be an obstacle to identifying it.


UARS positive patients, along with OSA positive patients are then referred for Nextgen Data Collection. UARS negative patients, along with all other patients, must also receive screening for insomnia and be given the Insomnia Severity Index “ISI” due to the frequency of the conditions coexisting and the potential negative health consequences.
Comorbid insomnia and sleep apnea “COMISA” are the most common co-occurring sleep disorders, with a global prevalence between 18% and 42%, and a prevalence between 29% and 67% among patients presenting for treatment. COMISA is associated with increased medical (eg, cardiometabolic conditions) and psychiatric morbidity (eg, mood disorders, post-traumatic stress disorder), and worse daytime functioning relative to each condition alone. As a result, clinical management of COMISA is often very challenging.14 Additionally a longer duration of insomnia is associated with a higher risk of incident diabetes.15 A new term, COMIUARS, is suggested for non OSA patients with UARS and comorbid insomnia.
Nextgen Data Collection is then broken down into three categories: structure, function, and behavior. This separation of data collection helps the clinician focus more on diagnosing the cause of the problem(s) and ultimately reveals 7 general treatment target areas (See figure 4).


There are so many types of treatments available, such as mandibular advancement devices “MADs”, positional therapy, upper airway surgery, and maxillomandibular osteotomy.16,17,18 The primacy of connecting the treatment options to the diagnosed cause(s) cannot be overstated. We need to focus less on the technologies available and more on specific ways to address the biologic compensations that are present.19
To help in this regard, each of the 7 treatment target areas are further broken down into subcategories (see figures 5,6,7,8,9,10,11,12) which have been shown to be responsive to specific treatments. Treatments and their specific targets are then graphically associated to help in treatment planning your patients.
Further research is needed to aid in diagnosis of specific compensations and associate them with the most effective treatments. In order to reach the entire population, and combat the high levels of undiagnosed disease, the data collection process must be simplified and cost effective.








Integrating SDB screening into dental practice represents a pivotal step toward bridging oral health and overall healthcare. Dentists and orthodontists are uniquely positioned to identify anatomical and behavioral risk factors for SDB, enabling early intervention that can prevent long-term systemic health complications.20 As dental professionals see their patients twice per year with a focus on the craniofacial respiratory structures, the field of dentistry is organically becoming the primary care platform for airway. From orthodontists and maxillofacial surgeons to otolaryngologists, from sleep medicine physicians to myofunctional therapists, the transdisciplinary approach is therefore the foundational element of the treatment algorithm used to treat these patients.21
By collecting data (structural, functional, behavioral) that relate to risk factors which contribute to the collapse of the airway, we are able to develop a rational approach to treatment choices. As our understanding of the complexities of airway and sleep grows, it becomes increasingly important to work with specialists from many disciplines to more predictably target and treat the cause of the problem and move forward from treating the severity of the disease.
This personalized sleep medicine strategy represents a transformative shift in healthcare, emphasizing individualized approaches to optimizing sleep health, considering the bidirectional relationship between sleep and health.22
References
Sankri-Tarbichi AG. Obstructive sleep apnea-hypopnea syndrome: Etiology and diagnosis. Avicenna J Med. 2012 Jan;2(1):3-8
Van Daele, M.; Smolders, Y.; Van Loo, D.; Bultynck, C.; Verbraecken, J.; Vroegop, A.; Lapperre, T.; Op de Beeck, S.;Dieltjens, M.; Vanderveken, O.M. Personalized Treatment for Obstructive Sleep Apnea: Beyond CPAP. Life 2024, 14, 1007
Young, T.; Palta, M.; Dempsey, J.; Skatrud, J.; Weber, S.; Badr, S. The occurrence of sleep-disordered breathing among middle-aged adults. N. Engl. J. Med. 1993, 328, 1230–1235
Benjafield AV, Ayas NT, Eastwood PR, Heinzer R, Ip MSM, Morrell MJ, Nunez CM, Patel SR, Penzel T, Pépin JL, Peppard PE, Sinha S, Tufik S, Valentine K, Malhotra A. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir Med. 2019 Aug;7(8):687-698
Oliver Vanderveken MD, Comparing CPAP to OAT; Clinical Effectiveness, Patients Preference, and Hypoxic Burden, AADSM 2025 Las Vegas, NV
Chen L., Pivetta B., Nagappa M., Saripella A., Islam S., Englesakis M., Chung F. Validation of the STOP-Bang Questionnaire for Screening of Obstructive Sleep Apnea in the General Population and Commercial Drivers: A Systematic Review and Meta-Analysis. Sleep Breath. 2021:1–11
Steve Lamberg DDS, Nextgen Data Collection, Nextgen Data Collection, AAPMD Podcast, April 2025
Peter Attia, Outlive, page 47, Vermilion Publishing, April 2023
Mike DeLuke DDS, MDS, Orthodontics 3.0 - A Proactive, Holistic Approach to Treatment, PAANNY Annual Meeting, New York, May 2025
Maggard MD, Sankari A, Cascella M. Upper Airway Resistance Syndrome. [Updated 2023 Jun 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan
Ogna A, Tobback N, Andries D, Preisig M, Vollenweider P, Waeber G, Marques-Vidal P, Haba-Rubio J, Heinzer R. Prevalence and Clinical Significance of Respiratory Effort-Related Arousals in the General Population. J Clin Sleep Med. 2018 Aug 15;14(8):1339-1345
Vizcarra-Escobar D, Duque KR, Barbagelata-Agüero F, Vizcarra JA. Quality of life in upper airway resistance syndrome. J Clin Sleep Med. 2022 May 01;18(5):1263-127
Tufik SB, Pires GN, Palombini L, Andersen ML, Tufik S. Prevalence of upper airway resistance syndrome in the São Paulo Epidemiologic Sleep Study. Sleep Med. 2022 Mar;91:43-50.
Ong JC, Crawford MR, Wallace DM. Sleep Apnea and Insomnia: Emerging Evidence for Effective Clinical Management. Chest. 2021 May;159(5):2020-2028.
Darraj A. The Link Between Sleeping and Type 2 Diabetes: A Systematic Review. Cureus. 2023 Nov 3;15(11
Randerath, W.; de Lange, J.; Hedner, J.; Ho, J.P.T.; Marklund, M.; Schiza, S.; Verbraecken, J. Current and novel treatment options for obstructive sleep apnoea. ERJ Open Res. 2022, 8, 00126-2022.
Verbraecken, J.; Dieltjens, M.; de Beeck, S.O.; Vroegop, A.; Braem, M.; Vanderveken, O.; Randerath, W. Non-CPAP therapy for obstructive sleep apnoea. Breathe 2022, 18, 220164.
Randerath, W.; Verbraecken, J.; de Raaff, C.A.; Hedner, J.; Herkenrath, S.; Hohenhorst, W.; Jakob, T.; Marrone, O.; Marklund, M.; McNicholas, W.T.; et al. European Respiratory Society guideline on non-CPAP therapies for obstructive sleep apnoea. Eur. Respir. Rev. 2021, 30, 210200.
German Ramirez, Guiding Craniofacial Growth and Development Through the Mouth to Give Better Airway, PAANNY Annual Meeting, New York, May 2025
H. Oh et al., Screening sleep-disordered breathing (SDB) in the everyday dental of ce− Pediatric and adult patients, Seminars in Orthodontics (2025
A. Huang et al., Surgical management of obstructive sleep apnea: A collaborative approach to a multidisciplinary disease, Seminars in Orthodontics (2025)
Garbarino, S.; Bragazzi, N.L.Revolutionizing Sleep Health: The Emergence and Impact of Personalized Sleep Medicine. J. Pers. Med. 2024, 14, 598.
As a practicing dentist for over 40 years, Steve Lamberg, DDS, DABDSM has been involved in providing treatment for snoring and sleep apnea using oral appliance therapy and managing patients' airways. He developed the Lamberg SleepWell Appliance and authored Treat the Cause... Treat the Airway: The Role of Snoring & Sleep Apnea in Contemporary Preventive Medicine.
Dr. Lamberg lectures nationally on topics including sleep apnea, airway management, and occlusion. He launched the Pediatric & Adult Airway Network of New York which exists to bring together all medical disciplines to encourage and support airway health. Their annual meeting is being held May 7-8, 2026 and details can be found here.

 | A guest post by
|